
Is there a Correlation between Excess Deaths and Levels of Vaccination by Local Authority in England?
Part 1 - analysis by Local Authority

Your support is very much appreciated. Please consider taking out a paid subscription to support independent journalism.
Subscriptions are best but if you would prefer to/ also like to buy me a coffee then click on the button below.


You will have no doubt read that, in many countries, excess deaths are massively up in 2022. I last wrote about it here.
In England there were over 1,623 excess deaths last week (18.7% up on the five year average) and 1,468 this week (up 16.7%). After a pandemic, you would expect fewer excess deaths with the most vulnerable sadly passing away during the pandemic itself. So why are there more deaths? The government doesn’t seem too interested in looking into it, so it is left to people like me to look at the data.
The Office of Health Improvement and Disparities produce a nice little dashboard which lets you view excess deaths in different ways. You can also download the data to play around with it.
One of the sections of the dashboard allows you to view excess mortality in England by Upper Tier Local Authority. You are able to view vaccination data by the exact same local authorities here. I thought it would be interesting to look at vaccination rates in each local authority and compare that with it’s excess mortality ratio.
To calculate excess mortality ratios I divided the number of registered deaths by the number of expected deaths. So, if the resulting number was 1, registered deaths were the same as expected deaths. Any number below 1 equals fewer deaths and any number above 1 equals more deaths.
I decided to look at all deaths since April of this year, since that is roughly when excess mortality started rising again. However, in a future article I may look further back in time.
Next, I recorded the percentage of the population in each local authority that had been vaccinated with a COVID-19 vaccine once, twice and three times. I then plotted the results on a scatter graph to see if there was any correlation.
The rest of this article is available as an early read for paid subscribers only. My articles take a lot of time to research and write so your support is very much appreciated and will ensure that I can continue to produce the same quality and quantity of articles going forwards.
In total there were 149 local authorities. I removed three outliers which reduced the total to 146 but, to be honest, that didn’t make too much of a difference.
The first graph compares excess mortality by vaccination rates in each local authority. Each blue dot is a separate local authority.
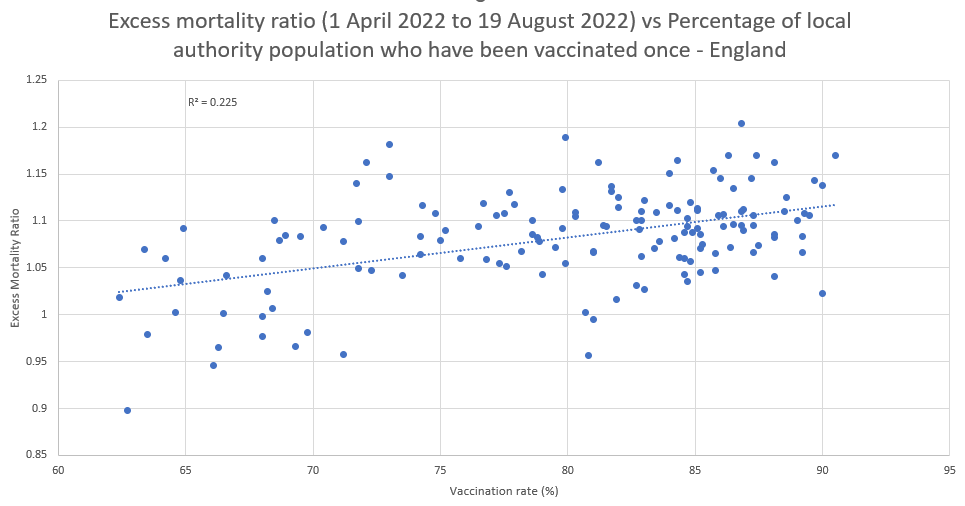
As you can see, the trendline is very firmly up, showing that as vaccination rates increase, so does excess mortality.
The R squared number is 0.225 meaning that between one fifth and one quarter of the excess mortality ratios can be predicted from the vaccination rates.
I also uploaded the data into pvalue.io to get a p-value (probability value) for the data. This gave a correlation coefficient of 0.474 and a p-value of <0.001 meaning there was a statistically significant correlation between the excess mortality ratio and vaccination rates.
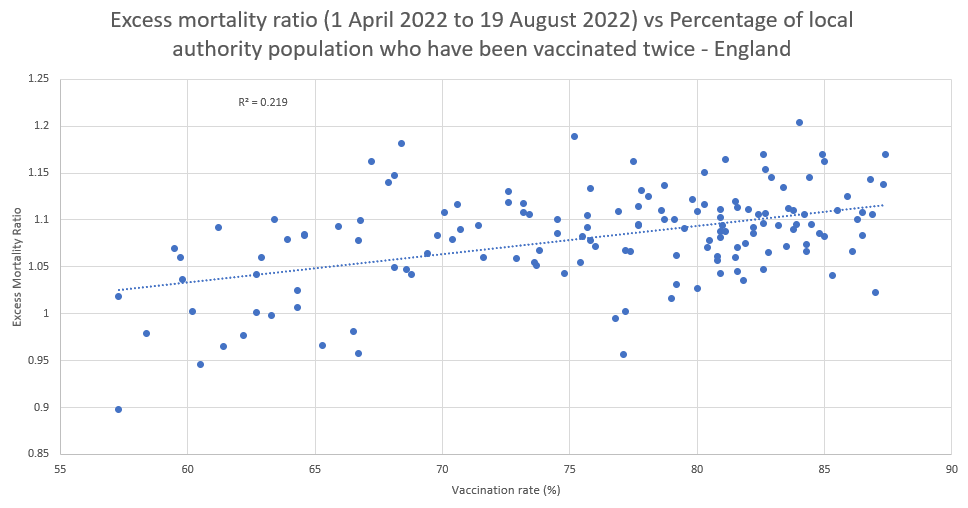
A similar result occurred when comparing two-dose vaccination rates with excess mortality. This time R squared was slightly lower at 0.219 and a correlation coefficient of 0.394. The p-value remained the same at <0.001, so again statistically significant.
For third doses, the trendline was still firmly up but with a R squared value of 0.1654. Correlation coefficient was 0.367 with another statistically significant p-value of <0.001.
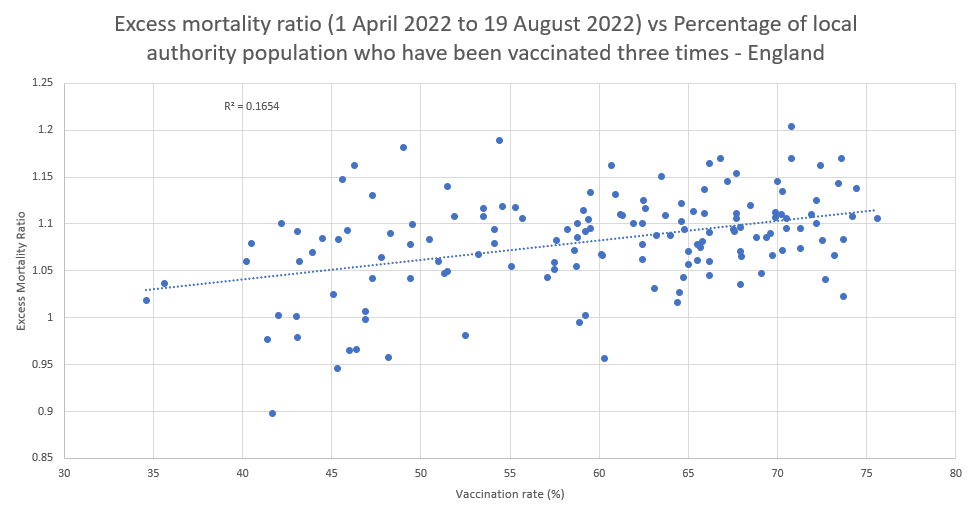
So it seems the strongest correlation is between whether you have ever been vaccinated and excess mortality, rather than the number of shots you have had.
Of course we have to remember that correlation doesn’t equal causation. Just because the number of lung cancer deaths correlate with the amount of people with matches in their pockets doesn’t mean that matches cause lung cancer.
There could be many reasons for this correlation. For example, local authorities with older populations are more likely to be vaccinated and other things are causing the excess deaths, e.g. lockdowns, long waits to access the health service. Another reason may be that healthier people decided not to get vaccinated and so are less likely to die from whatever is causing the excess mortality rates to rocket.
However, it is an interesting correlation and one that should not be ignored. Hopefully, people with better statistical skills than I have can have a look at the data, tear it apart and tell me why the excess mortality is occurring. I am merely presenting an observation after my hypothesis. All the data is there for anyone to interrogate and tell me that I’ve gone about it completely the wrong way or that there may be something in it. That is how real science works.
Subscriptions are best but if you would prefer to/ also like to buy me a coffee then click on the button below.
Attempts to ask these questions of various datasets are vitally important and you have found a really great resource to apply your questions, and to replicate other's findings. It is a lot of good effort. For which many are grateful, as there is clearly a danger signal for one or more shots.
Here are my impressions:
With all of these analyses published on a variety of Substacks, when trying to look at number of jabs, mortality and correlations, there is always the problem of sampling from the population without replacement. In other words, once you have killed off a number of people with the first shot, it is a different sample for the second shot. Some of the most vulnerable were taken out. Some of the people who took one shot and decided against the second might have had a bad reaction and decided, "whoa no more for me." Or maybe they started to see bad news trickle in. For example, my sister fortunately decided against the shot after seeing three people in her social and work circle promptly pass away after their one or two shots. At some point they stopped refrigerating the shots to be so cold. Other groups have verified bad lots and serious problems and variation in manufacturing. The same thing then happens again between shot 2 and 3 and 3 and 4 to further winnow and change the nature of the remaining sample. This would attenuate the correlation a bit for shot two, and then even more for shot three as you have now taken out more people from the same population who potentially had highest vulnerability to these shots if in fact that is a thing.
Ideally you want three separate populations to test, randomized or well-matched to compare separately 1, 2 and 3 shot schemes. Given the sampling without replacement and the other variables adding possible variation to the outcome including inaccuracies in reporting of shots it is remarkable that these signals are still so strong, as death is the dependent variable. The findings so far still supports the recommendation that all shots should be stopped immediately and all data sifted through.
Of course, all this work should have been done by pharma prior to FDA authorization, a randomized set of trials.
So there may be sophisticated techniques to help overcome, post hoc, these biases in the sampling. I think Matthew Crawford might have referred to progressive bias in sampling as survivor bias. There are also regression techniques in the area of survival analysis that might apply--who survives the shot schemes the longest, what makes them different using independent variables related to your overall theory and/or supplied by critics?
A comprehensive analysis with these sorts of multiple data sets across populations and the work of many thoughtful analysts is due--maybe as a coordinated roundtable with steering committee to plan and then conduct analyses. Also, if someone has access to graduate students in statistics or population public health data analysis it seems like this type of work would be ideal to that setting, as the project would be a layered, iterative, programmatic and complex set of questions. Such could be the focus of a master's or dissertation thesis with oversight of a large and qualified committee, including outside members who have been active on these questions and datasets. (I've been a member of about 2 dozen dissertation oversight committees and 4 master's theses).
Who wouldn't want "The Naked Emperor" as one of a committee to sign off on their thesis?
I'd recommend you make this article immediately free to all (currently has 7 day paywall which is fine on other articles for sure) and ask people to circulate on Social Media asking for evidence and analysis for support or refutation.